Health
Fillers vs Facelift Surgery: When Is It Time to Consider the Real Thing

For many people, dermal fillers feel like the perfect answer to the first signs of ageing. They are quick, require virtually no downtime, and deliver a subtle, refreshed appearance without the commitment of surgery. But there comes a point for a growing number of patients when top-ups no longer produce the results they once did, and the conversation inevitably shifts toward something more permanent. So how do you know when it is time to move from the syringe to the scalpel?
If you have been wondering whether facelift surgery is the right next step for you, understanding the fundamental differences between these two approaches and recognising the signals your face may already be sending can help you make a more informed, confident decision.
What Fillers Can (and Cannot) Do
Dermal fillers, most commonly made from hyaluronic acid, are injectable substances that add volume, smooth fine lines, and enhance facial contours. They work exceptionally well in the early stages of ageing, particularly when volume loss in the cheeks, temples, or under-eye area is the primary concern. Results are immediate and the treatment typically takes under an hour. Understanding the benefits of facelift surgery compared to these temporary measures is what ultimately helps patients decide when the time for a more lasting change has arrived.
However, fillers address only one dimension of facial ageing: volume. They cannot reposition sagging tissues, tighten loose skin along the jawline or neck, or lift descended fat pads. Knowing the best age to get a facelift and recognising when your face has moved beyond what fillers can correct is one of the most important conversations to have with a specialist. As one leading plastic surgeon has noted, the concept of adding enough filler volume to compensate for loose skin rather than surgically tightening it is a popular but ultimately flawed notion. Misuse of fillers over time can result in bloated cheeks that lack normal definition, impaired facial expression, and distorted proportions that no longer look naturally youthful.
There is also the matter of longevity. Fillers typically last between six and twenty-four months depending on the product and the area treated, meaning they require ongoing maintenance. Many patients find that, over several years, the cumulative cost of repeated filler appointments can rival or even exceed the one-time investment of facelift surgery in London.
The Six Signals It Is Time to Consider Surgery
Knowing when to make the transition is not always straightforward, but there are clear indicators that non-surgical treatments may no longer be sufficient.
1. Jowls and jawline definition have been lost. When the lower face begins to sag and jowls form, fillers are unable to provide meaningful correction. Surgical lifting repositions deeper tissues to restore a sharper, more defined jawline something injectables simply cannot replicate.
2. Loose skin in the neck. Significant neck laxity, including visible vertical bands and hanging skin below the chin, falls firmly outside the capabilities of fillers. A full or lower facelift, combined with a neck lift where necessary, is the most effective intervention.
3. You are booking top-ups more and more frequently. If you find yourself returning every few months just to maintain the same look and the results still do not feel quite right it is a strong sign that structural ageing has progressed beyond what volume replacement can address. Facelift surgery, by contrast, resets the clock in a way that holds for years rather than requiring constant upkeep.
4. Your face looks heavy or overfilled. At a certain point, relying solely on injectables can actually accentuate heaviness or distort natural facial proportions. If well-meaning top-ups have left your face looking fuller but not fresher, surgery may provide the more natural, long-lasting result you are seeking.
5. Deep nasolabial folds and significant skin laxity. Fillers can soften these folds to a degree, but they fall short when laxity is advanced. A deep plane or SMAS technique releases the underlying ligaments, repositions the tissue layers, and allows the skin to settle in a naturally rejuvenated position without the telltale tightness of older surgical methods.
6. You are ready for a long-term solution. Facelift surgery turns back the clock approximately ten years, and with proper skincare and occasional injectables for maintenance, many patients require only one procedure in their lifetime.
Understanding the Ageing Process
Facial ageing is not simply about wrinkles. Gravity, volume loss, and the weakening of facial ligaments work together to transform the round or oval face of youth into a squarer, heavier shape with age. The oval becomes rectangular. The cheekbones appear flatter. The jawline softens into jowls. This structural shift is what fillers are ill-equipped to fully reverse and it is precisely what facelift surgery is designed to correct.
Understanding when the right time for surgery arrives is equally nuanced. There is no single correct answer. Most patients undergo facelift surgery between their late forties and early sixties, when the signs of structural ageing become prominent enough to warrant surgical correction. However, candidacy depends far more on skin quality, facial anatomy, and the degree of tissue sagging than on chronological age alone. Some patients in their early forties with more advanced early ageing will benefit from surgery sooner, while others in their late sixties remain excellent candidates for the first time.
Choosing the Right Type of Facelift
One of the most important aspects of the facelift journey is understanding that the procedure is not a single, one-size-fits-all operation. The technique recommended will depend on the extent of ageing, the areas of primary concern, and the patient’s goals and recovery expectations.
Mini facelift: Ideal for patients in their late thirties to early fifties experiencing early jowl formation and mild skin laxity in the lower face. It uses smaller incisions, involves less downtime, and produces results that typically last five to ten years. It is an excellent entry point for those whose ageing has progressed beyond what fillers can address, but who do not yet require a comprehensive lift.
SMAS facelift: The SMAS (Superficial Musculoaponeurotic System) technique tightens the underlying facial muscles and tissue as well as repositioning the skin. It offers a natural, rejuvenated appearance while addressing sagging in the lower face and neck, and tends to produce results lasting around seven to ten years.
Deep plane facelift: Widely regarded as the gold standard in facial rejuvenation, the deep plane technique releases facial ligaments and repositions the deeper muscle layers as a single unit. Unlike older surface lifts, it avoids the stretched or ‘windswept’ look and creates a beautifully natural, long-lasting result typically ten to fifteen years. It is best suited to patients with more advanced ageing changes.
Fillers and Facelifts: Not Mutually Exclusive
It is worth noting that fillers and facelift surgery are not competing choices they are complementary tools used at different stages of the ageing journey. Many facelift patients continue with occasional filler treatments after surgery to maintain skin smoothness and address fine lines that surgery alone does not target. The combination of structural surgical correction and well-placed injectables for maintenance is, for many patients, the most comprehensive and sustainable approach to long-term facial rejuvenation.
One important caveat: emerging research suggests that a history of repeated, panfacial filler injections may have implications for future facelift surgery. Studies have identified potential associations between cumulative filler use and complications including compromised tissue vascularity and altered longevity of the lifting effect. This makes early surgical consultation all the more valuable your surgeon can assess your tissue quality and advise on timing before extensive filler accumulation becomes a consideration.
Finding the Right Surgeon in London
If you have reached the point where you are seriously considering facelift surgery, choosing your surgeon carefully is arguably the most important decision you will make. London and Harley Street in particular is home to some of the most experienced facelift specialists in the world.
The best facelift surgeon in London will be one whose practice is centred primarily on facial procedures, who can demonstrate consistent, natural-looking results across a range of techniques, and who takes the time during consultation to understand your individual anatomy, concerns, and expectations. Specialisation matters enormously in facial surgery; a surgeon performing thousands of facelifts over a career develops a level of nuance and precision that generalists cannot match.
When researching facelift London options, prioritise surgeons who are on the GMC Specialist Register for plastic or facial surgery, who operate in CQC-regulated facilities, and who are transparent about what each technique can realistically achieve. Patient testimonials, before-and-after galleries, and independent review platforms offer valuable insight but nothing replaces an in-person consultation where you can ask direct questions and assess the rapport.
Whether you are considering a mini facelift in London, a comprehensive deep plane procedure, or are simply at the research stage, the most important step you can take right now is to speak with an expert. A well-timed, well-executed facelift does not replace your face it reveals the best version of it.

Medical practices today are under more administrative pressure than ever. Between patient scheduling, insurance verification, follow-up calls, and endless paperwork, front-office staff are often stretched too thin and hiring another full-time in-house employee isn’t always practical. This is exactly why a growing number of clinics, private practices, and healthcare providers are turning to a healthcare virtual assistant for support.
What Is a Healthcare Virtual Assistant?
A healthcare virtual assistant is a remote professional who handles administrative and support tasks for medical practices, without being physically present in the office. Unlike a general virtual assistant, a health virtual assistant is typically trained to understand healthcare-specific workflows, appointment systems, patient intake processes, and basic medical terminology.
This makes them a practical middle ground between hiring additional in-house staff and letting administrative backlogs pile up.
Common Tasks a Healthcare Virtual Assistant Handles
- Scheduling and rescheduling patient appointments
- Answering routine patient calls and emails
- Sending appointment reminders and follow-ups
- Managing patient intake forms and basic data entry
- Coordinating between departments or referring physicians
- Handling insurance verification paperwork
- Supporting billing and coding teams with administrative prep work
By taking these repetitive tasks off the plate of clinical and front-desk staff, practices free up time for what actually matters, patient care.
Why Practices Are Hiring Medical Virtual Assistants
1. Lower Overhead Costs
Hiring a full-time, in-office administrative employee comes with costs beyond salary equipment, office space, benefits, and training. A virtual assistant reduces much of this overhead while still providing reliable support.
2. Flexible Scheduling
Many practices don’t need a full 40-hour front-desk employee; they need coverage during specific hours or peak call times. Virtual assistants can be hired part-time or scaled up as patient volume grows.
3. Reduced Administrative Burnout
Front-desk staff juggling too many responsibilities are more prone to burnout and errors. Delegating repetitive tasks to a health virtual assistant helps existing staff focus on higher-priority, in-person patient interactions.
4. Faster Response Times
Patients expect quick responses to calls and messages. A dedicated virtual assistant can manage inboxes and phone lines more consistently, reducing missed calls and delayed follow-ups.
What to Look for When Hiring a Medical Virtual Assistant
If you’re considering hiring a medical virtual assistant for your practice, keep these points in mind:
- Relevant experience: Prior experience in a medical or healthcare administrative setting is a strong plus
- Familiarity with your scheduling/EHR software: Reduces onboarding time significantly
- Clear communication skills: Since they’ll often be the first point of contact for patients
- Confidentiality awareness: Healthcare-related roles require a strong understanding of handling sensitive patient information responsibly
- Trial period: Start with a smaller scope of tasks to evaluate fit before expanding responsibilities
Is a Healthcare Virtual Assistant Right for Your Practice?
If your front desk is overwhelmed, patients are waiting too long for callbacks, or you’re considering another in-house hire purely for administrative relief, a healthcare virtual assistant may be worth exploring. It’s a flexible way to add capacity without the long-term commitment and cost of a full-time employee.
Frequently Asked Questions
What does a healthcare virtual assistant do? They typically manage scheduling, patient communication, data entry, and administrative support remotely, allowing in-office staff to focus on direct patient care.
Is hiring a virtual assistant safe for handling patient information? Practices should ensure any virtual assistant they work with follows appropriate confidentiality and data-handling practices, and that any tools or platforms used meet the practice’s compliance requirements.
Can a virtual assistant work part-time for a medical practice? Yes, many practices hire virtual assistants for specific hours or peak periods rather than full-time coverage, which offers flexibility as patient volume changes.
Final Thoughts
Administrative overload is one of the most common, and most avoidable, sources of stress in medical practices today. A healthcare virtual assistant offers a practical, cost-effective way to keep operations running smoothly without adding the overhead of another full-time in-house hire.
If you’re exploring reliable, pre-vetted virtual assistant support for your practice, Virtual Assistants Pakistan connects healthcare providers with remote assistants suited to administrative and patient-support needs.

There is a new growth industry in American healthcare, and it is not a drug, a device, or an app. It is checking. In the space of two years, the United States government has built one of the largest audit operations in its history, aimed squarely at the private insurers that deliver public health coverage to more than thirty million older Americans.
The numbers tell the story quickly. The federal audit workforce for this programme has grown from roughly forty reviewers to around two thousand certified medical coders. Audits that once trickled out have moved to a quarterly rhythm. Artificial intelligence now helps reviewers read medical records at speed, though humans make the final calls. And when auditors find errors in a sample of patient files, they no longer just correct the sample. They extrapolate the error rate across the entire contract and demand the difference back.
For British readers accustomed to NHS headlines, the scale takes a moment to absorb. This is a government checking whether it overpaid private companies, with hundreds of billions of dollars a year in play.
Why the checking became necessary
The programme under the microscope is called Medicare Advantage. Instead of the government paying doctors and hospitals directly, private insurers receive a monthly sum for each member they cover, adjusted for how ill that member is. A member whose records show diabetes, heart failure, and kidney disease brings a higher payment than a healthy one. The logic is sound: sicker people cost more to care for, and insurers should not be punished for covering them.
The vulnerability is equally clear. The payment follows what is recorded, not what is treated. Over fifteen years, an industry grew up around maximising the recording. Insurers hired teams and bought software to re-read years of old medical files, hunting for conditions that could be added to a member’s record. Every addition raised the member’s risk score, and the monthly payment with it.
Independent congressional advisers now estimate the resulting excess payments at tens of billions of dollars a year. In March 2026, government auditors published reviews of three insurance plans and found that between 81 and 91 percent of sampled high-risk diagnosis codes lacked proper supporting evidence in the medical records. The same month, the US Department of Justice concluded a 117.7 million dollar settlement with a major insurer whose chart-review programmes, prosecutors argued, added diagnoses by the thousand while almost never removing a wrong one.
The machinery of the response
The audit programme itself, known as RADV, for Risk Adjustment Data Validation, is where the government’s answer lives, and its recent expansion is the real news. A useful plain-language account of the Medicare Advantage audit expansion sets out what changed: audits of payment year 2020 began in February 2026, samples per contract now range from 35 to 200 members depending on plan size, insurers get a five-month window to produce the medical records behind each audited diagnosis, and the whole cycle repeats every quarter rather than every few years.
The genuinely novel element is extrapolation. Under the old regime, an insurer caught with unsupported codes repaid only the specific errors found. Under the new one, a 40 percent error rate in a sample becomes a 40 percent clawback across the contract. The change converts audits from a nuisance into an existential financial event, which is precisely the point.
Insurers have responded the way regulated industries always do when the referee starts counting properly: they are professionalising in a hurry. Compliance teams that once assembled audit responses from spreadsheets and email chains are buying purpose-built platforms. Review programmes that only ever added diagnoses are being rebuilt to remove unsupported ones too, because prosecutors made one-directional review the signature of bad faith.
The view from this side of the Atlantic
Britain does not run Medicare Advantage, but it is not a spectator to the underlying question. The NHS increasingly allocates funds using population-need formulas built on recorded data, and integrated care systems are experimenting with outcome-linked payment. Wherever documentation determines allocation, the American lesson applies: the data will drift toward the money unless verification keeps pace.
There is also a procurement lesson. British health bodies buying data and AI systems from an increasingly global vendor market can borrow the questions American auditors now ask. Can every automated conclusion be traced to its evidence? Does the system correct errors in both directions, or only the profitable one? Could a third party reconstruct the decision three years later?
The Americans learned to ask those questions after the money was gone. The audit army, the quarterly cadence, and the nine-figure settlements are what catching up looks like. The cheaper option, available to anyone still designing their systems, is to ask them at the start.
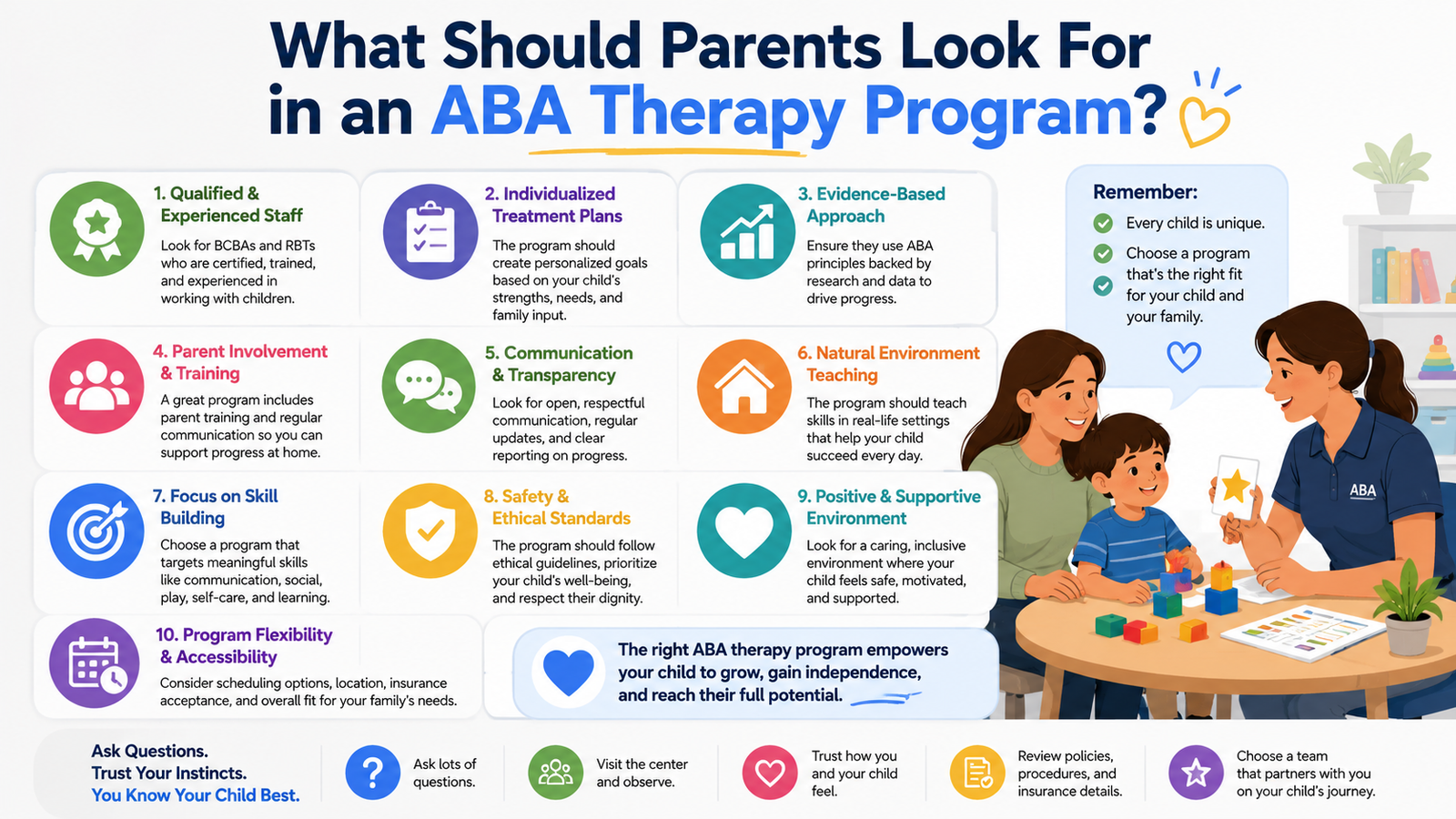
My friend spent about four months researching all of the best ABA programs for her son. She made a spreadsheet. She compiled all of the information that programs provided to her in a folder that was color-coordinated and very beautifully organized.She even had up to 23 websites open in her browser at a time researching.Yet in the end, she confessed to me that even after all of that research, she wasn’t even really sure if she had been asking the right questions.
I still remember my friend describing the 4 months she spent researching for her 4 year old son with autism before entering a first ABA clinic.Four months of an in depth research of ABA programs, with an Excel spread sheet, a thick folder color coded by topic, and at times 23 browser tabs open on her computer. And even then, she would say she was not sure if she had asked the right questions.
So let’s cut through it.
Evaluating the therapy environment.
Take a walk through of the area before committing to a program would be ideal. Do a tour of the area and then sit down with a few families and have them give you a tour of their “clinic” or area where work takes place. Ask them to sit with you and explain how things work. Then sit in on a session with their lead therapist. Ask the staff members what they are doing at any given time while physically in the area with kids. Are they processing data and managing in the back or are they sitting right next to the kids working with them. How does a session deal with a crisis? Is there any warmth in the area or is it a processing area and kids and families just go there to have work done. There are still some really great clinical settings where kids and families feel really supported and at home and work is being done and there are other settings that feel sterile, cold and just like a “therapy” area where kids go to receive processing. Just because something looks different on the outside doesn’t mean it’s not great.
Here are a few things to pay attention to when looking at a therapeutic setting:
- Low noise and visual clutter in core learning spaces (sensory overwhelm is real)
- Natural light, or at minimum, lighting that doesn’t buzz
- Clear zones for different types of activities, not one generic room where everything happens
- Staff who make eye contact with the kids, not just the clipboards
That last one sounds small. It isn’t.
What’s the turnover rate?
Everyone asks whether therapists are BCBA-certified — and yes, that matters enormously, Board Certified Behavior Analysts have rigorous training requirements and any program worth considering should have BCBAs supervising the work — but I’ve watched parents spend twenty minutes asking about credentials without ever
What’s the turnover rate?
So here’s the follow-up question that nobody ever asks: What is the average amount of time that a therapist stays with a program before leaving for another job?This is a very important question for parents to ask because of how vital consistency is to a child’s progress in ABA therapy.ABA is a very relationship-driven process, and it takes a long time for a child to build up enough trust with a therapist in order to have a successful relationship.If a child is making great progress with a particular therapist, only to have that therapist leave for another job three months later, it can be very frustrating and even defeating for a child.So it is very important for parents to ask about turnover in a program before deciding whether or not to go with that program. A good program will not be embarrassed to tell you about how long their average therapist stays.
What are the credentials of the staff at the program? It is very important to have therapists, consultants and other supervisory staff that are BlockPlaceholderZZ3
- BCBA or BCaBA certification for supervisors and lead therapists
- Registered Behavior Technicians (RBTs) who have completed proper training (not just a weekend course)
- Ongoing supervision hours, not just an initial sign-off
- Experience specific to your child’s age group and needs
Individualized plans, not template therapy
However, I have found that there are many clinics that really do put the best practices of ABA to use, and really can change a child’s life for the better.As I mentioned before, every child with autism is different, and each will have their own individual way of communicating, their own individual sensory needs, and their own individual way of life.In the creation of the best plan for a child’s ABA goals, the therapist would use the best practices for the individual child, using the individual child’s methods of communication, and individual child’s ways to manage sensory issues.A truly effective ABA program would not use a single set of methods or protocol for all skills for all children.Instead, the most effective ABA programs for children with autism will be those that are tailored to the individual child, using a variety of different ABA methods, that best meet the child’s individual needs.An example of a less effective program, would be a clinic, that uses only one type of communication with all of the children, and has all of the children do all of their skills in one type of activity.This type of program could drag a child through life, having the child crawl to complete a skill, in order to complete his or her ABA therapy, and could be very dehumanizing to the child.
A good ABA program for your child should also have individually written goals that apply to your child’s actual life. For example, before starting ABA with your child, you should be able to view a detailed assessment of your child. In particular, your child’s goals for ABA should reflect his or her current situation and be relevant to his or her daily life.As a general rule, your child’s ABA goals for ABA should be to acquire a series of functional skills that any normally developing 2- to 6- year old child would acquire in order to interact with family and others in the community.These skills might include for example being able to cross the room, being able to stack blocks, being able to engage in cooperative play with others, and so on.Therefore, prior to starting a program of ABA with your child, you should view a detailed assessment of your child, and then review your child’s written goals for ABA in order to ensure that the goals of ABA are relevant to your child.
(One small indicator of this sort of program is if they can tell you within the first 5-10 minutes of your first intake meeting what your child’s goals will be. In reality, Individualized Programs take time to develop).
Here is a graphic to compare typical ‘individualized’ ABA programs and what ABA really should look like for children and their families.
| Generic program approach | Individualized program approach |
| Same starting goals for most new clients | Goals built from a comprehensive intake assessment |
| Progress measured on a fixed schedule | Data reviewed continuously and plans adjusted regularly |
| Family gets updates occasionally | Family is part of the team from day one |
| Therapy stays in the clinic | Skills are practiced across home and community settings too |
Family involvement isn’t optional
The best ABA programs involve the families of the children with Autism Spectrum Disorders in the process of developing and implementing a treatment plan to help their child succeed. The staff of these ABA programs can equip the child’s therapists with strategies and tools that can be used at home by family members, in schools by teachers and other school staff, and in community settings by peer models and others. Families can learn new ways of communicating with children with Autism Spectrum Disorders, and tools to deal with difficult situations. Also, there are many things that children with Autism Spectrum Disorders can learn in their ABA sessions that will be very useful to their families.
However, if parent training is not included as a core component of treatment then this is an area that you should really push to get the program to acknowledge as a “gap” in their services.
The aba therapy bedford ma team at Bierman Autism Centers in the area for parents doing their research for a family-centered model of ABA for their child with autism is the model that comes to mind for staff to treat families with the respect and dignity that any family deserves.
16 One last thing — and I mean this one
Trust your gut. There are many things that can feel right or wrong to different people. We can’t always even explain to ourselves why we think a particular program would be good for our child. We may be misreading a program that is really good for our child because of our anxiety about our child. But, we can also trust our gut and know that a program does not feel right for our child. And, it is very important to pay attention to your gut if a program makes you feel like a nuisance for asking questions, if the answers to your questions sound rehearsed, and if you leave a meeting with a lot of confusion and uncertainty. These are all red flags and your gut is trying to tell you something. Pay attention to your gut. Your child deserves better.
A program can look great on paper and be a disaster. Don’t let a fancy intake process fool you. Your child deserves a program that earns your trust and has your child’s best interest at heart.
Your child needs a program that is worthy of your trust and does everything to earn it. An attractive intake packet does not equal a quality program.

Top 5 Online Marriage Counselling Websites in UK For NRIs

Elmwood Park Slip and Fall Lawyer: Protecting Your Rights After a Serious Injury

How Publication Services Support Authors and Researchers From Draft to Publication
Who Is Shameera? All You Need To Know About Charli XCX’s Mother
Who Is Gulliver Flynn Oldman? The Untold Story of Sir Gary Oldman’s Son
Meet Rosemary Turner: The Mother of Actor Callum Turner
-
 Biographies5 months ago
Biographies5 months agoWho Is Shameera? All You Need To Know About Charli XCX’s Mother
-
 Biographies4 months ago
Biographies4 months agoWho Is Gulliver Flynn Oldman? The Untold Story of Sir Gary Oldman’s Son
-
 Biographies5 months ago
Biographies5 months agoMeet Rosemary Turner: The Mother of Actor Callum Turner
-
 Biographies5 months ago
Biographies5 months agoWho is Todd McRae? Meet Tate McRae’s Father
-
 Celebrity5 months ago
Celebrity5 months agoWho Is Peter Hernandez? The Real Story of Bruno Mars’ Father
-
 Biographies3 months ago
Biographies3 months agoWho is Alexandra James? Inside The Life of Jeremy Clarkson’s Former Partner
-
 Biographies5 months ago
Biographies5 months agoWho Is Alvin Martin? All About the Whoopi Goldberg’s First Husband
-
 Biographies4 months ago
Biographies4 months agoWho Is Daniel Mara? The Untold Story of Kate Mara’s Private Sibling